By Danielle Wehle, MD
Educational dermpath case series for dermatology residents
Patient: 70-year-old man
Lesion Location: Back
A biopsy of an acute blistering eruption on the back was performed. Take a moment to review the histologic images below — what’s your diagnosis?
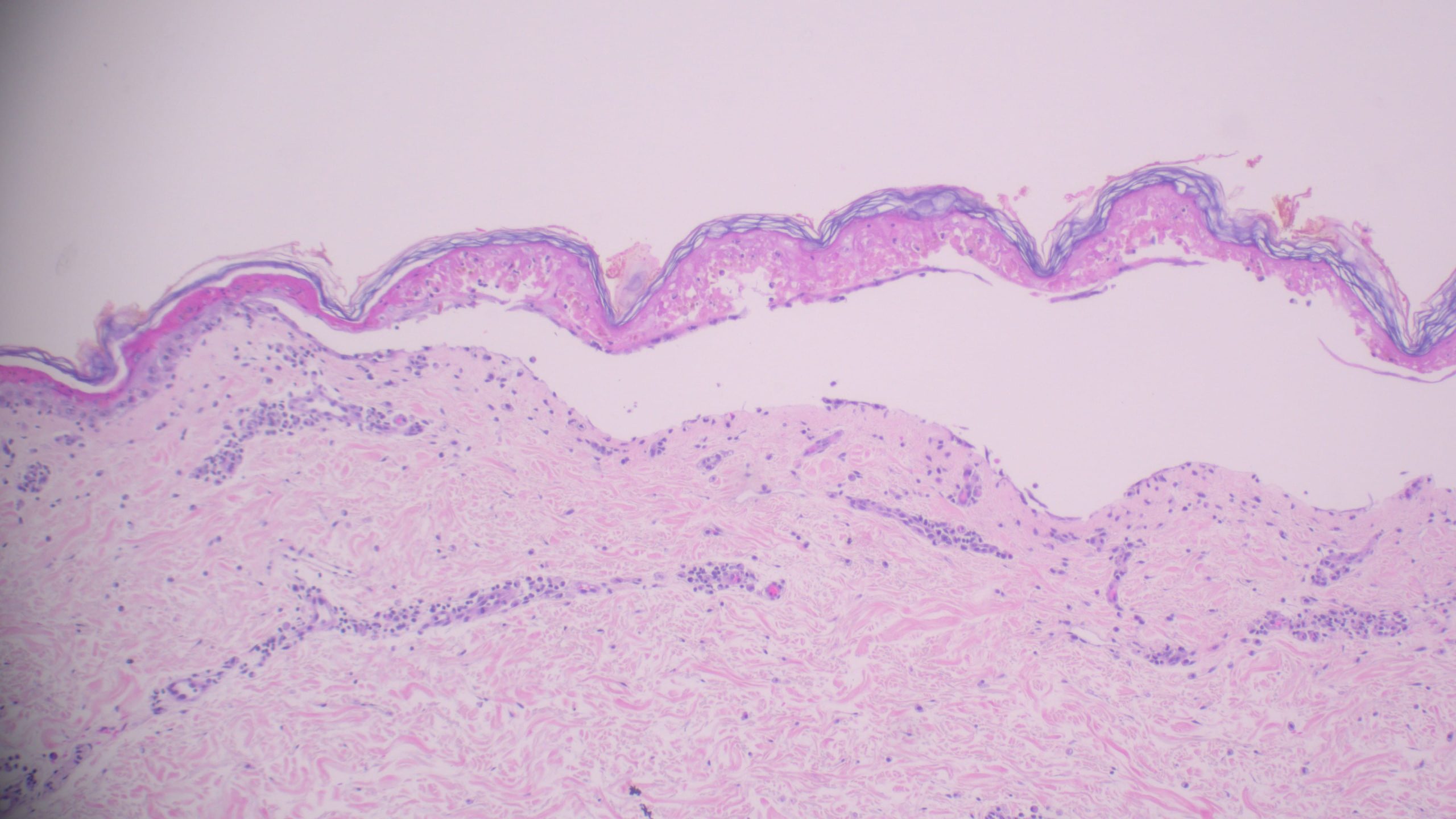
(Low-power histologic view of blistering lesion)
Key Histologic Findings
On examination, several defining features stand out:
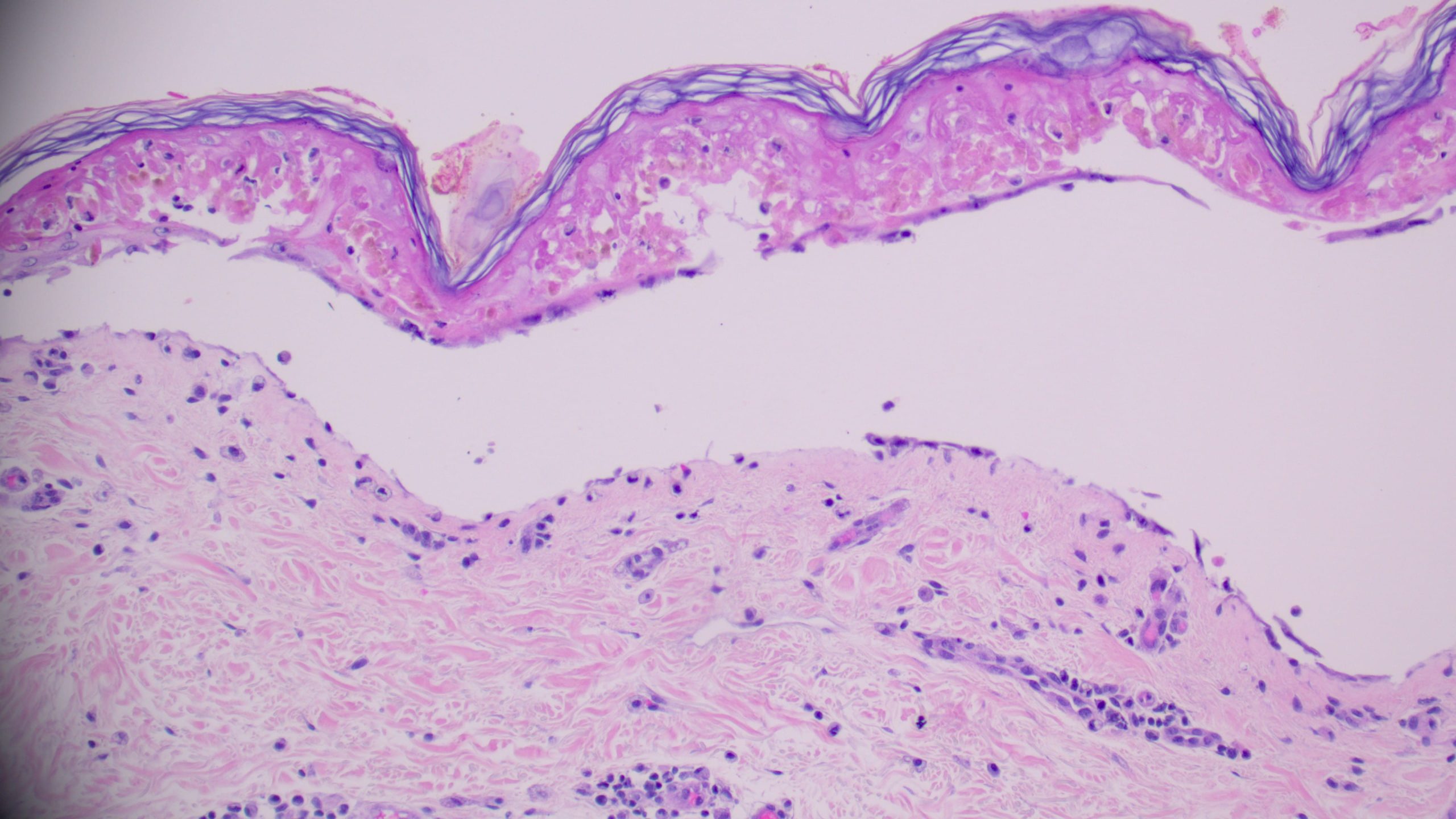
(Medium power showing full-thickness epidermal necrosis and subepidermal split)
Differential Diagnosis: Three Common Mimickers
When evaluating a blistering disorder such as this, several entities in the differential diagnosis come to mind. Let’s walk through the three most likely contenders and highlight what sets them apart.
1️⃣ Paraneoplastic Pemphigus
Etiology: Associated with underlying malignancy (most often lymphoma or thymoma); autoantibodies target desmosomal proteins including desmoplakins
Histology:
Key Distinction:
Paraneoplastic pemphigus and TEN both feature keratinocyte necrosis, but paraneoplastic pemphigus shows suprabasal acantholysis and a more prominent inflammatory infiltrate. TEN, by contrast, shows full-thickness epidermal necrosis with minimal inflammation and no acantholysis.
2️⃣ Staphylococcal Scalded Skin Syndrome (SSSS)
Etiology: Exfoliative toxins A and B from Staphylococcus aureus cleave desmoglein 1, causing superficial epidermal splitting
Histology:
Key Distinction:
The critical differentiator is the level of the split. SSSS shows superficial acantholysis at the granular layer, while TEN demonstrates full-thickness necrosis with a subepidermal blister. Age is also a helpful clinical clue: SSSS predominantly affects young children, while TEN is more common in adults and is typically drug-induced.
3️⃣ Acute Graft-versus-Host Disease (GvHD)
Etiology: Donor T-cell-mediated attack on recipient epithelium following allogeneic bone marrow or stem cell transplantation
Histology:
Key Distinction:
Acute GvHD and TEN can overlap clinically and histologically in severe cases. However, GvHD classically shows interface dermatitis with lymphocytic infiltrate and satellite cell necrosis rather than the pauci-inflammatory full-thickness epidermal necrosis that defines TEN. Clinical history — particularly a recent transplant — is essential.
The Final Diagnosis:
Toxic Epidermal Necrolysis (TEN)
The combination of full-thickness epidermal necrosis, subepidermal blistering, and minimal dermal inflammation is diagnostic of TEN. This is a life-threatening disorder most commonly triggered by a medication, often beginning with a flu-like prodrome before progressing to widespread epidermal sloughing involving more than 30% of body surface area. Immediate withdrawal of the offending drug is critical.
Key Takeaways for Residents:
Clinical history is non-negotiable: recent medications, transplant history, or known malignancy each significantly shift the differential.
(Diagnostic high-power image: full-thickness epidermal necrosis with minimal inflammation)
📚 Quick Summary
| Feature | Toxic Epidermal Necrolysis | Paraneoplastic Pemphigus | Staph Scalded Skin Syndrome | Acute GvHD |
| Full-thickness necrosis | ✅ Present | ❌ Absent | ❌ Absent | ❌ Absent |
| Subepidermal blister | ✅ Present | ✅ May be present | ❌ Intraepidermal | ❌ Absent |
| Acantholysis | ❌ Absent | ✅ Suprabasal | ✅ Granular layer | ❌ Absent |
| Inflammation | ❌ Minimal | ✅ Prominent | ❌ Variable | ✅ Interface |
| Behavior | Life-threatening | Serious | Self-limited | Serious |
💬 Final Thought
TEN is one of dermatopathology’s most urgent diagnoses. The triad of full-thickness necrosis, subepidermal blistering, and sparse inflammation tells the story quickly at the microscope. Remember: minimal inflammation with maximal destruction? Think TEN.
Sagis Diagnostics is proud to support dermatology residents and dermatology residency programs through high-quality educational content and histopathologic learning resources.
Follow us on Instagram for more micro-learning opportunities with interactive cases and pathology insights.