By Alison Messer, MD
Educational dermpath case series for dermatology residents
Patient: 73-year-old woman
Lesion Location: Groin
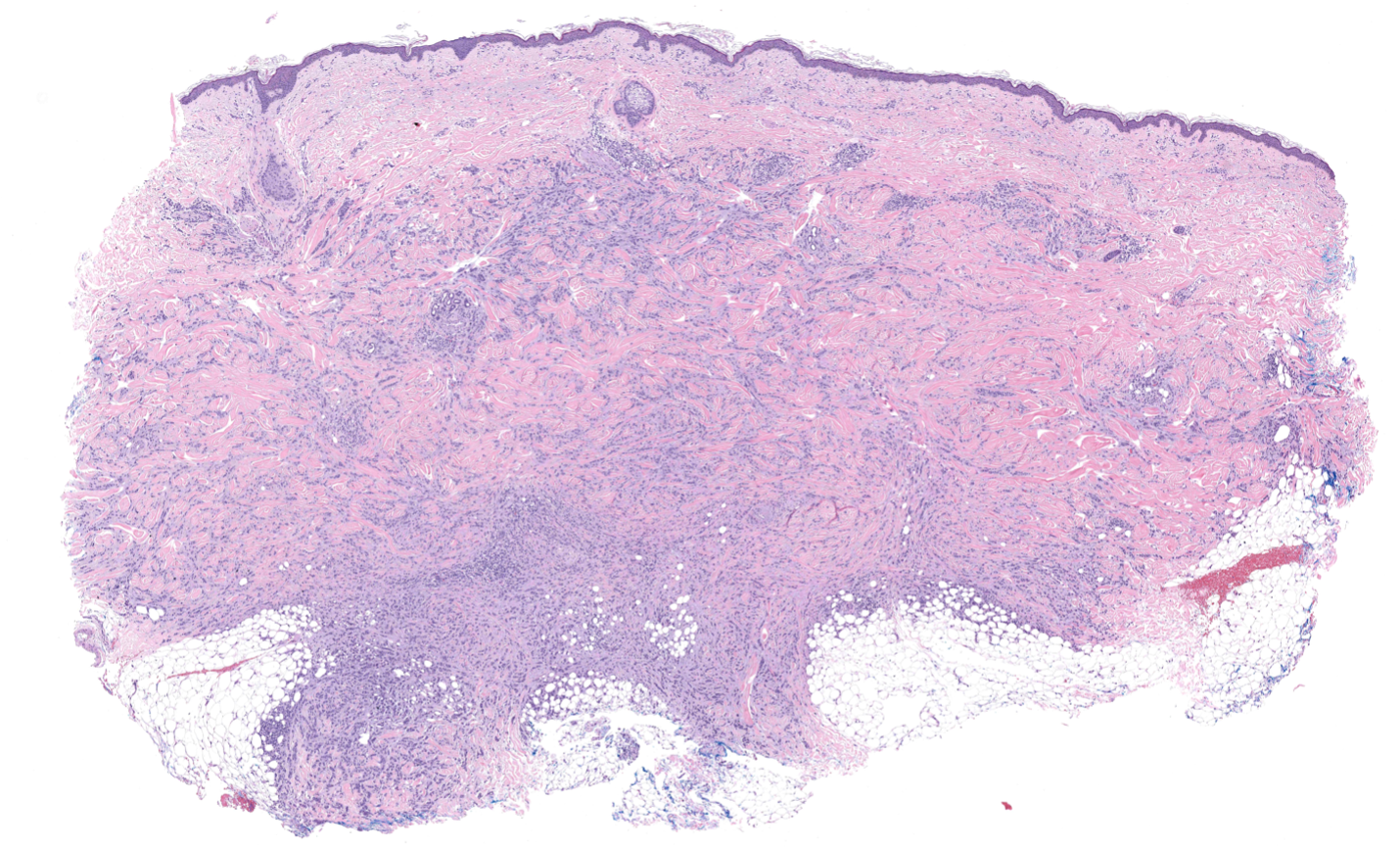
A biopsy of pink papules and nodules from the groin was performed. Take a moment to review the histologic images below — what’s your diagnosis?

Key Histologic Findings
On examination, several defining features stand out:
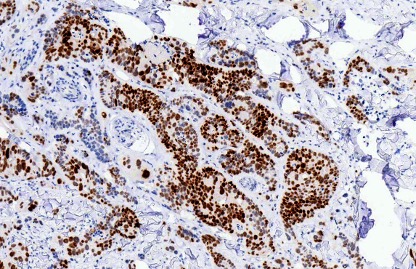
(CDX-2)

(CK-20)
Differential Diagnosis: Three Common Mimickers
When evaluating an atypical basaloid lesion in the skin, the differential diagnosis includes both primary cutaneous tumors and metastatic lesions. Let’s walk through the three most likely contenders and highlight what sets them apart.
1️⃣ Merkel Cell Carcinoma
Etiology: Merkel cell polyomavirus (MCPyV) or UV-induced carcinogenesis; neuroendocrine origin
Histology:
Key Distinction:
Although Merkel cell carcinoma and metastatic colorectal carcinoma both exhibit CK20 positivity and a basaloid appearance, Merkel cell carcinoma lacks duct formation and is CDX2 negative. The perinuclear dot-like pattern of CK20 staining and positivity for neuroendocrine markers (synaptophysin, chromogranin) confirm a diagnosis of Merkel cell carcinoma.

(Merkel cell carcinoma)
2️⃣ Basal Cell Carcinoma
Etiology: UV-induced mutations in the hedgehog signaling pathway (PTCH1); most common skin malignancy
Histology:
Key Distinction:
While basal cell carcinoma shares the basaloid cell morphology, it is readily distinguished by its negative CK20 and CDX2 immunoprofile. Peripheral palisading and stromal retraction artifact are hallmarks of BCC not seen in metastatic colorectal carcinoma. The absence of “dirty” necrosis and duct formation further argues against a colorectal primary.

(Basal cell carcinoma: peripheral palisading and stromal retraction)
3️⃣ Metastatic Breast Carcinoma
Etiology: Invasive breast carcinoma with cutaneous metastasis; most commonly invasive ductal carcinoma
Histology:
Key Distinction:
Metastatic breast carcinoma can closely mimic colorectal carcinoma when ductal structures are present. The IHC profile is the key separator: breast carcinoma is typically CK7 positive, and negative for CK20 and CDX2. Metastatic colorectal carcinoma shows the reverse pattern, making a targeted IHC panel essential.
(Metastatic breast carcinoma: basaloid cells infiltrating the dermis)
The Final Diagnosis:
Metastatic Colorectal Carcinoma
The combination of basaloid cells, duct formation, and “dirty” necrosis is highly characteristic of colorectal origin. Immunohistochemistry confirms CK20 and CDX2 positivity, supporting gastrointestinal origin and ruling out other entities in the differential diagnosis. In the context of a cutaneous metastasis from the groin in a 73-year-old woman, these findings together are diagnostic.
Key Takeaways for Residents:
(Diagnostic high-power view: duct formation with “dirty” necrosis)
📚 Quick Summary
| Feature | Metastatic Colorectal Carcinoma | Merkel Cell Carcinoma | Basal Cell Carcinoma | Metastatic Breast Carcinoma |
| HPV-related | ❌ No | ❌ No | ❌ No | ❌ No |
| Basaloid cells | ✅ Present | ✅ Present | ✅ Present | ❌ Variable |
| Duct formation | ✅ Present | ❌ Absent | ❌ Uncommon | ✅ Present |
| “Dirty” necrosis | ✅ Present | ❌ Absent | ❌ Absent | ❌ Absent |
| CK-20 positive | ✅ Yes | ✅ Yes | ❌ No | ❌ Typically No |
| CDX-2 positive | ✅ Yes | ❌ No | ❌ No | ❌ No |
| CK-7 positive | ❌ Typically No | ❌ No | ❌ No | ✅ Typically Yes |
| Behavior | Metastatic | Aggressive / metastatic | Locally aggressive | Aggressive / metastatic |
💬 Final Thought
Metastatic colorectal carcinoma is a classic dermatopathology “look-alike” that rewards careful microscopic examination and a disciplined IHC approach. Remember: the dirty necrosis and CDX2 tell the story.
Sagis Diagnostics is proud to support dermatology residents and dermatology residency programs through high-quality educational content and histopathologic learning resources.
Follow us on Instagram for more micro-learning opportunities with interactive cases and pathology insights.