By Dr. Danielle Wehle, Sagis Diagnostics
Educational dermpath case series for dermatology residents
Patient: 20-year-old female
Lesion Location: Trunk
A biopsy was performed of a diffuse rash on the trunk of this young woman. Take a moment to review the histologic images below to see how Dr. Wehle arrived at this diagnosis.
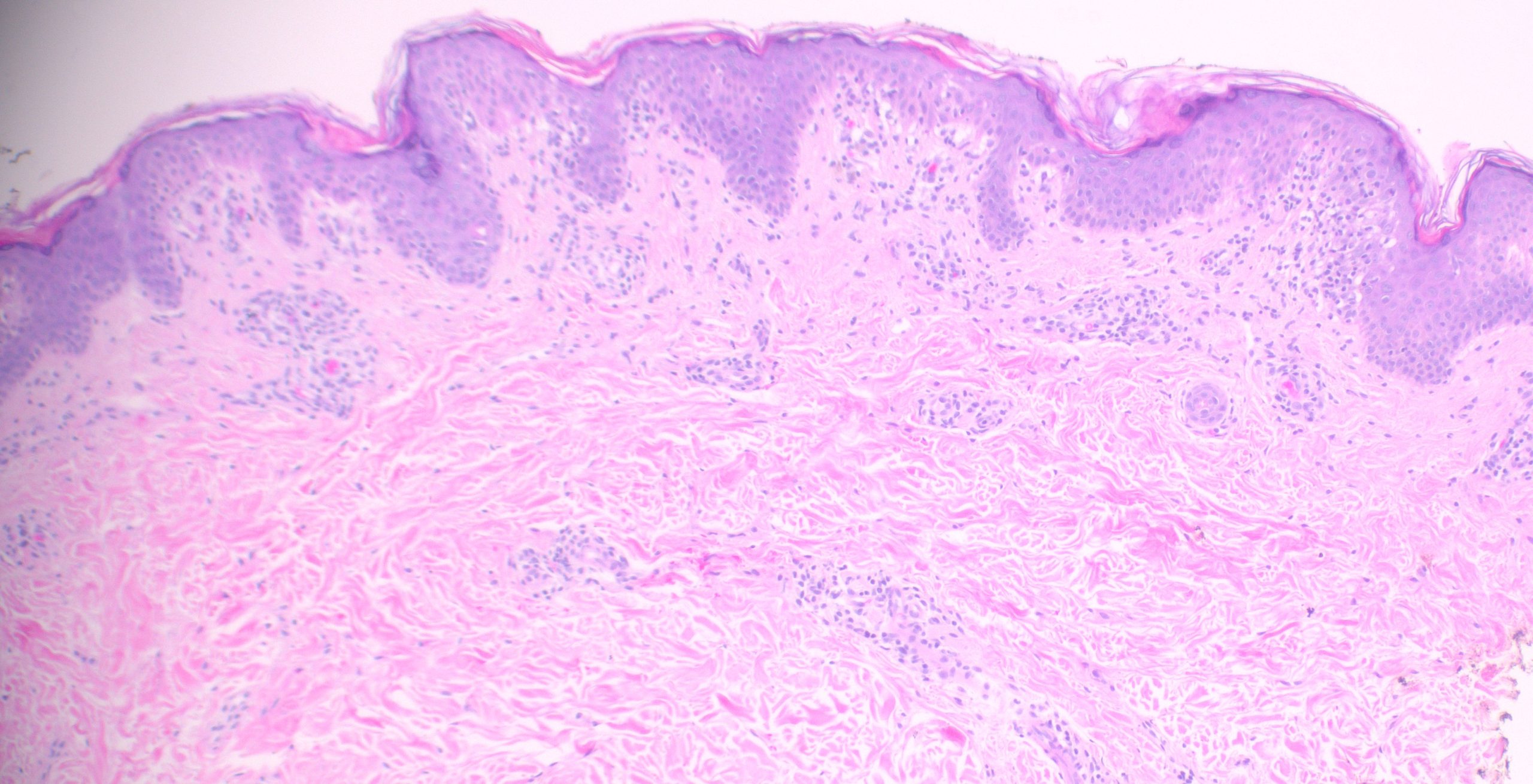
(Low-power histologic view of diffuse rash biopsy)
On examination, several defining features stand out:
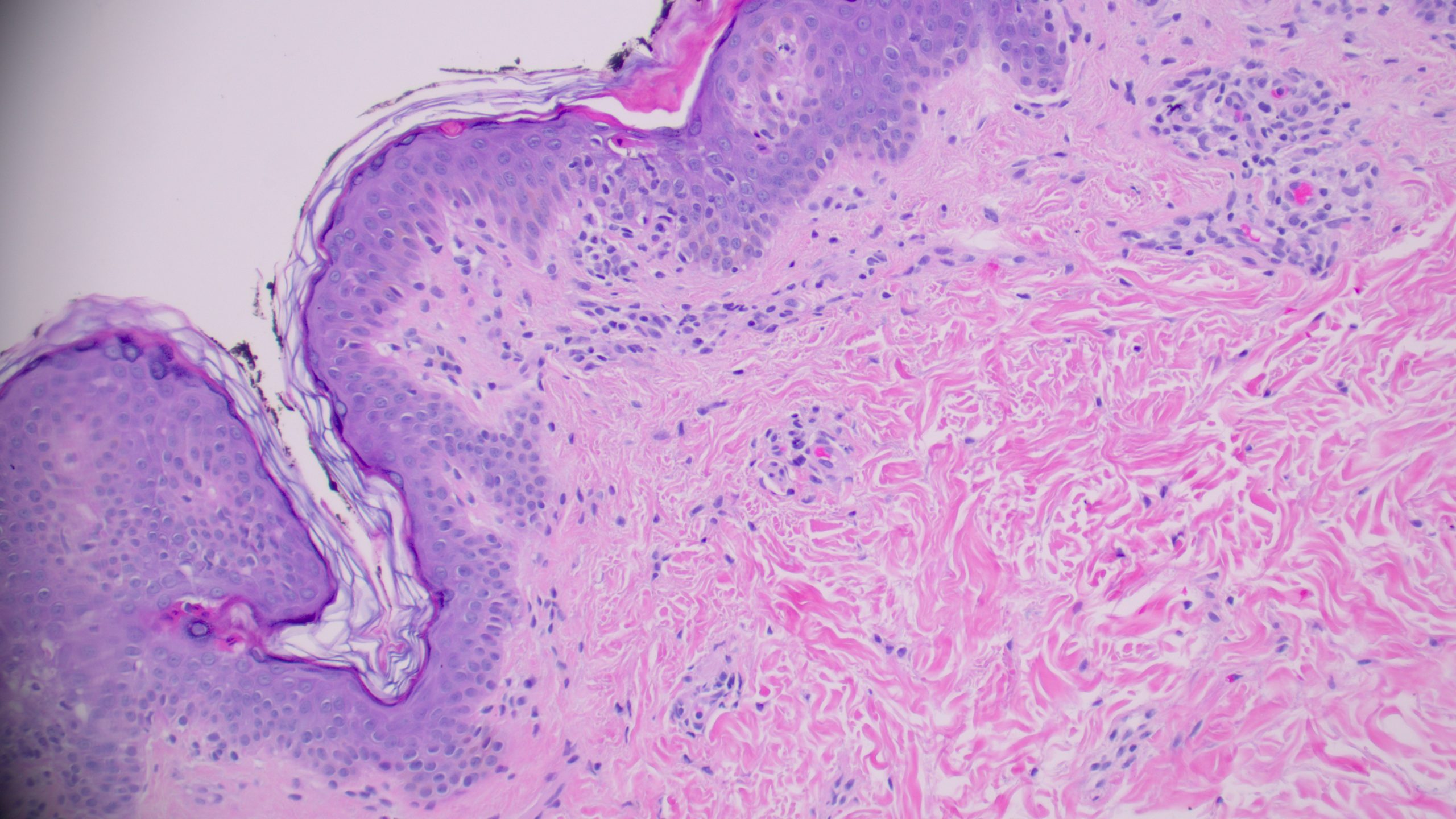
(Medium power showing wedge-shaped perivascular lymphocytic infiltrate)
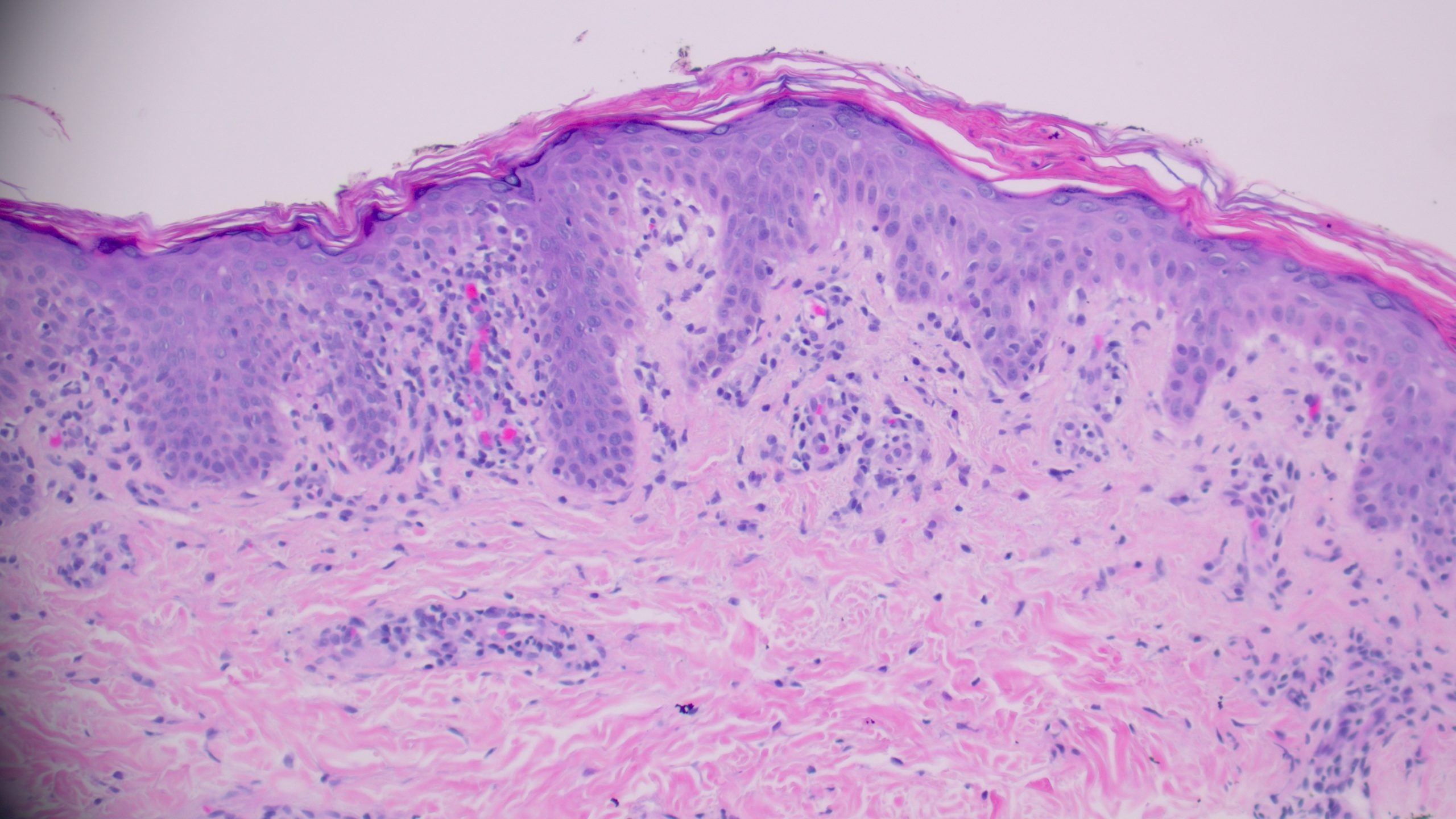
(High power showing necrotic keratinocytes and erythrocyte extravasation into the epidermis)
When evaluating a papular rash with a wedge-shaped infiltrate like this, several differentials come to mind. Let’s walk through the three most likely contenders and highlight what sets them apart.
1️⃣ Fixed Drug Eruption
Etiology: Hypersensitivity reaction to a medication; reproducible at the same anatomic site with re-exposure
Histology:
Key Distinction:
Fixed drug eruption can be confused with PLEVA due to overlapping interface changes, but the presence of prominent band-like interface dermatitis and melanin pigment deposition are characteristic of FDE. Critically, erythrocyte extravasation into the epidermis — a hallmark of PLEVA — is absent in fixed drug eruption.
Etiology: Local hypersensitivity reaction to insect or arthropod venom/saliva
Histology:
Key Distinction:
Both arthropod bite reactions and PLEVA display a wedge-shaped perivascular infiltrate, making them architectural mimickers. However, arthropod bites show numerous eosinophils and do not have necrotic keratinocytes in the epidermis. In PLEVA, eosinophils are not a significant feature, and epidermal damage is defining.
Etiology: Recurrent, self-healing CD30+ T-cell lymphoproliferative disorder; low-grade malignancy with benign behavior
Histology:
Key Distinction:
Lymphomatoid papulosis shares a wedge-shaped infiltrate and self-limited papular course with PLEVA, making histologic distinction critical. The key differentiator is the presence of large atypical cells that are CD30 positive in LyP — absent in PLEVA, which is comprised predominantly of CD8 positive T-lymphocytes. Furthermore, LyP does not show the prominent epidermal changes of PLEVA. Immunohistochemistry is essential when this differential is on the table.
Pityriasis Lichenoides et Varioliformis Acute (PLEVA)
The combination of a wedge-shaped perivascular lymphocytic infiltrate, necrotic keratinocytes in the epidermis with overlying parakeratosis, and erythrocyte extravasation into the epidermis and superficial dermis is diagnostic of PLEVA. This triad, together with the clinical picture of a young patient with a diffuse papular rash on the trunk, clinches the diagnosis. PLEVA commonly affects patients under 30 years of age, with lesions involving the trunk and proximal extremities presenting as red-brown, mildly pruritic papules that may form blisters, crusts, or ulcers.
Key Takeaways for Residents:
| Feature | PLEVA | Fixed Drug Eruption | Arthropod Bite Reaction | Lymphomatoid Papulosis |
| Wedge-shaped infiltrate | ✅ Yes | ❌ No | ✅ Yes | ✅ Yes |
| Necrotic keratinocytes | ✅ Present | ❌ Absent | ❌ Absent | ❌ Absent |
| Erythrocyte extravasation | ✅ Present | ❌ Absent | ❌ Absent | ❌ Absent |
| Eosinophils | ❌ Absent | ❌ Variable | ✅ Prominent | ❌ Absent |
| CD30+ atypical cells | ❌ No | ❌ No | ❌ No | ✅ Yes |
| Melanin pigment | ❌ No | ✅ Common | ❌ No | ❌ No |
| Behavior | Benign / self-limited | Benign (drug reaction) | Benign | Low-grade lymphoma |
PLEVA is a classic dermatopathology “wedge-shaped mimic” that rewards careful microscopic examination at every power level. Remember: the triad of wedge-shaped infiltrate + epidermal necrosis + erythrocyte extravasation tells the story — and immunohistochemistry closes the case when LyP is in the differential.
Sagis Diagnostics is proud to support dermatology residents and dermatology residency programs through high-quality educational content and histopathologic learning resources.
Follow us on Instagram for more micro-learning opportunities with interactive cases and pathology insights.