By Thomas Davis, MD, FAAD
Educational dermpath case series for dermatology residents
Patient: 69-year-old female
Lesion Location: Right rib cage and left hip
Take a moment to review the clinical and histologic images below to see how Dr. Davis arrived at this diagnosis.
Clinical Presentation: One-year history of asymptomatic, bilaterally distributed erythematous patches on the trunk
A biopsy of the patch lesion was performed to establish a definitive diagnosis.

On examination, several defining features stand out:
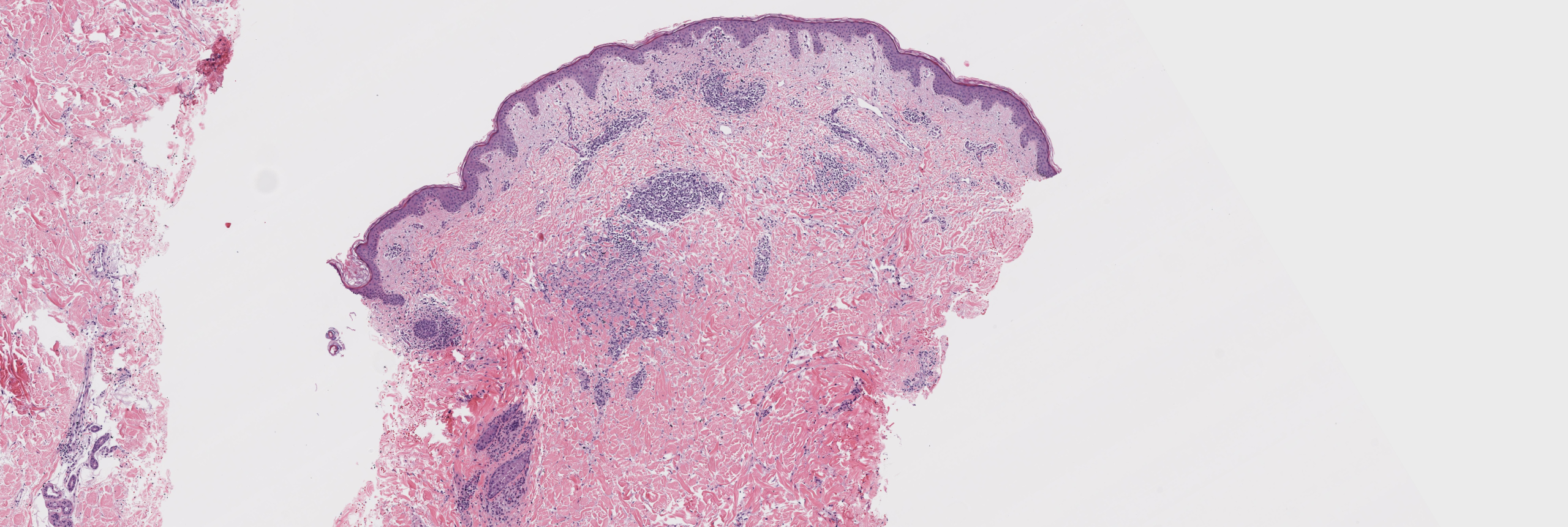
[Image 1: Low-power histologic view showing subtle interstitial infiltrate]
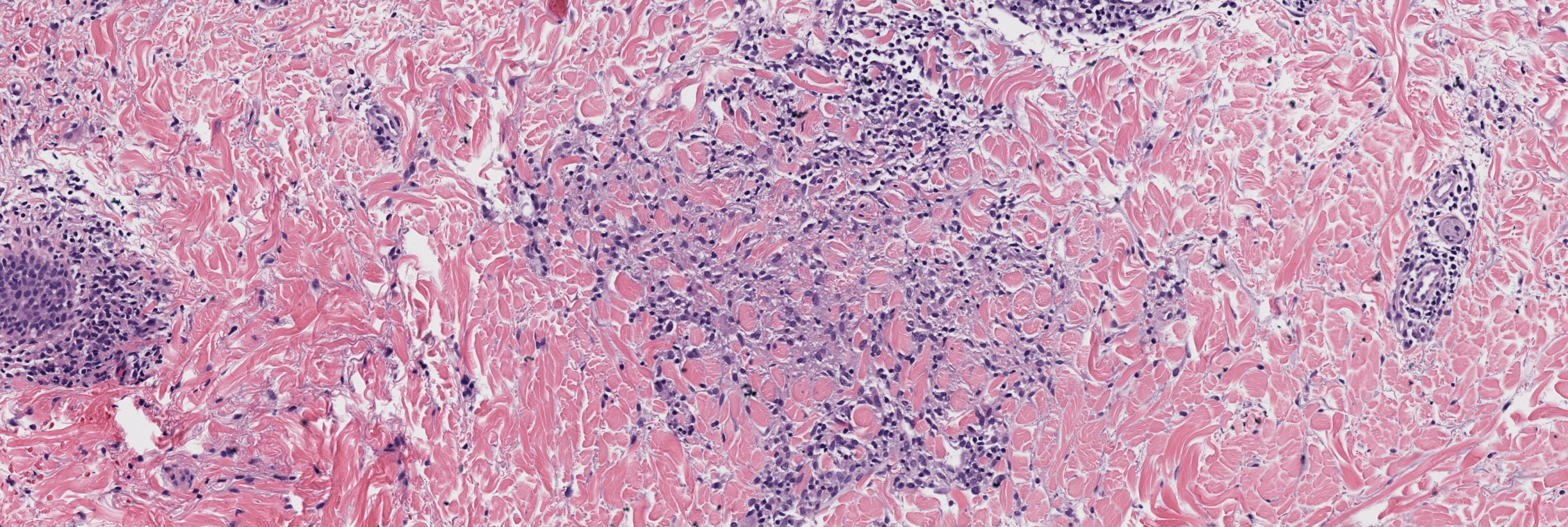
[Image 2: Medium power showing interstitial lymphohistiocytic infiltrate]
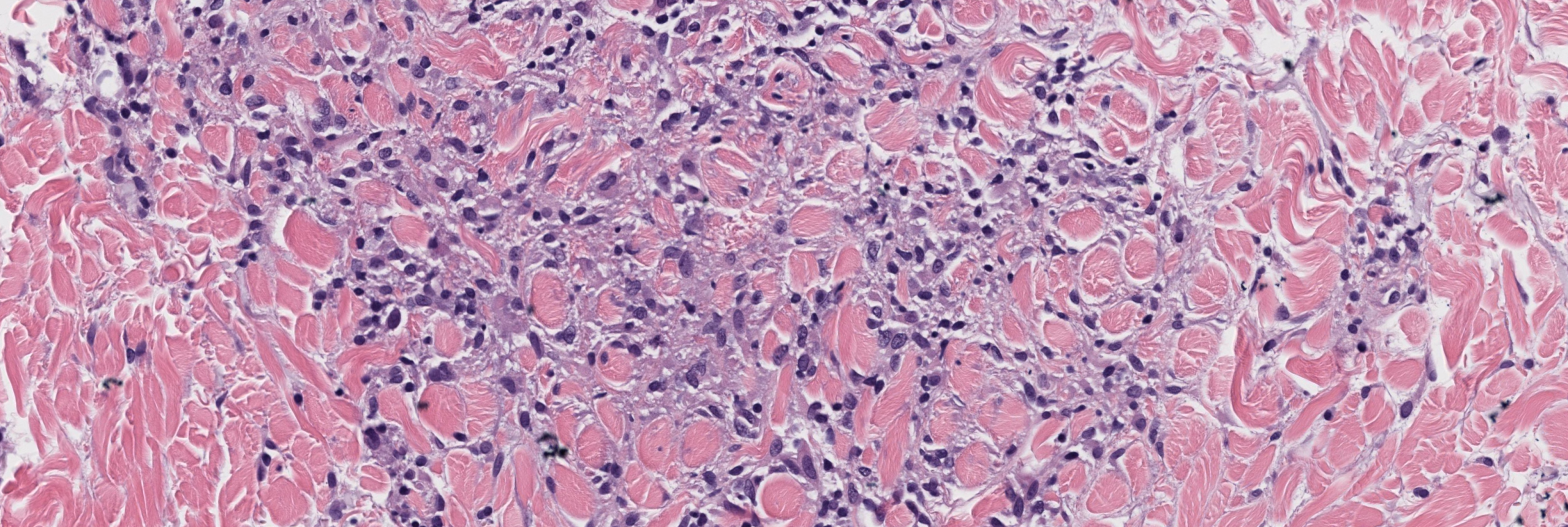
[Image 3: High power showing histiocytes and increased dermal mucin between collagen bundles.]
When evaluating an interstitial dermatosis like this, several differentials come to mind. Let’s walk through the 3 most likely contenders and highlight what sets them apart.
Etiology: Cutaneous T-cell lymphoma with interstitial growth pattern presenting in early patch stage
Histology:
Key Distinction:
While both entities show interstitial infiltrates, interstitial MF displays atypical lymphocytes with hyperchromatic, cerebriform nuclei. Patch GA shows bland histiocytes rather than atypical lymphocytes, and lacks epidermotropism. The clinical context is also critical—MF patches are often more extensive and may show progression over time.
Etiology: Early-stage morphea with prominent inflammatory infiltrate preceding dermal sclerosis
Histology:
Key Distinction:
Inflammatory morphea characteristically shows plasma cells within the infiltrate and early signs of dermal sclerosis with collagen bundle thickening and straightening, particularly in the deep dermis. Patch GA lacks plasma cells and does not show collagen alteration or sclerosis. Instead, histiocytes are seen “splitting” between normal-appearing collagen bundles with associated mucin.
Etiology: Reaction pattern associated with autoimmune diseases (rheumatoid arthritis, lupus), infections, or medications
Histology:
Key Distinction:
IGD displays a denser histiocytic infiltrate with characteristic neutrophils and nuclear debris creating a “dirty” appearance, along with obvious collagen degeneration. Patch GA shows a more subtle, cleaner interstitial infiltrate of bland histiocytes with prominent mucin deposition and intact, well-preserved collagen bundles. IGD is also more commonly associated with underlying systemic diseases.
Patch-Type Granuloma Annulare
This is patch-type granuloma annulare, an uncommon but increasingly recognized variant of classic GA. The diagnosis is confirmed by the interstitial pattern of bland mononuclear histiocytes dissecting between preserved collagen bundles with increased dermal mucin and absence of epidermal changes or palisaded granulomas.
[Image: High-power view highlighting bland histiocytes within collagen with mucin stain inset]
📚 Quick Summary
| Feature | Patch GA | Interstitial MF | Inflammatory Morphea | IGD |
| Infiltrate composition | Bland histiocytes | Atypical lymphocytes | Lymphocytes + plasma cells | Dense histiocytes + neutrophils |
| Dermal mucin | ✅ Prominent | ✅ Can be present | ❌ Minimal | ❌ Absent/minimal |
| Epidermal changes | ❌ Absent | ✅ Epidermotropism (variable) | ❌ Absent | ❌ Absent |
| Collagen alteration | ❌ Preserved bundles | ❌ Normal | ✅ Sclerosis/thickening | ✅ Degeneration |
| Plasma cells | ❌ Absent | ❌ Rare | ✅ Prominent | ❌ Rare |
| Neutrophils/debris | ❌ Absent | ❌ Absent | ❌ Absent | ✅ Present |
| Palisading | ✅ May be present | ❌ Absent | ❌ Absent | ✅ May be present |
| Behavior | Benign | Malignant | Benign/inflammatory | Reactive/secondary |
💬 Final Thought
When you see subtle interstitial histiocytes with mucin but no obvious granulomas, don’t dismiss granuloma annulare from your differential—you might just be looking at its stealthier patch variant. Remember: not all GA makes rings, and not all patches are lymphoma!
Follow us on Instagram for more micro-learning opportunities with interactive cases and pathology insights.
Sagis Diagnostics is proud to support dermatology residents and dermatology residency programs through high-quality educational content and histopathologic learning resources.
📖 Reference:
Khanna U, North JP. Patch-type granuloma annulare: Clinicopathologic study of 23 cases with increased dermal mucin. J Cutan Pathol. 2020;47(7):614-622.



