By Dr. Vickers, Sagis Diagnostics
Educational dermpath case series for dermatology residents
Patient: 17-year-old male
Lesion Location: Diffuse hypopigmented patches across the body
This biopsy is from a 17-year-old male patient with white patches present for 2 years at the time of biopsy. Take a moment to review the clinical and histologic images below, do you know how Dr. Vickers came to this diagnosis?
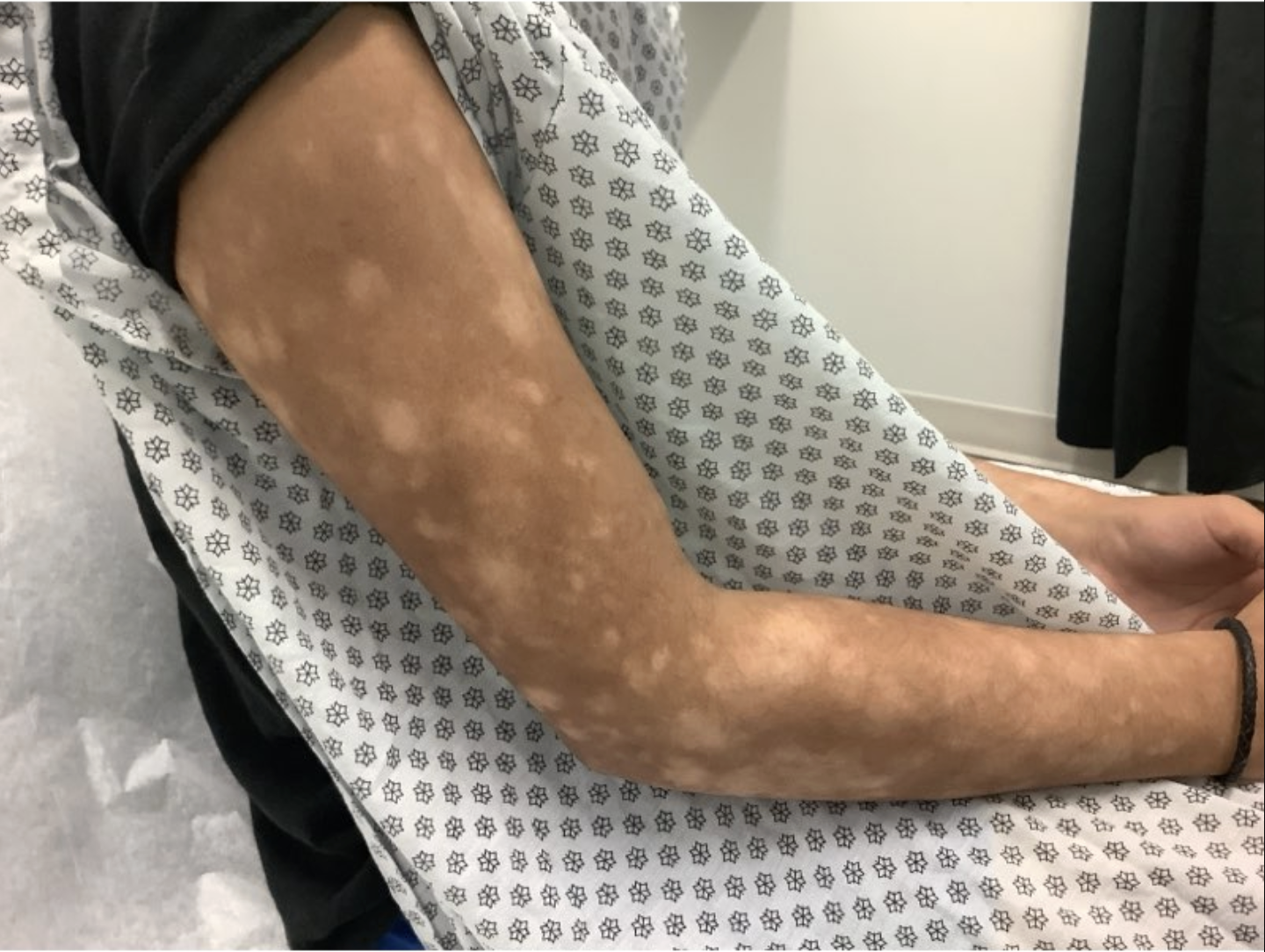
(Image 1: Clinical photo — hypopigmented patches on patient’s skin)
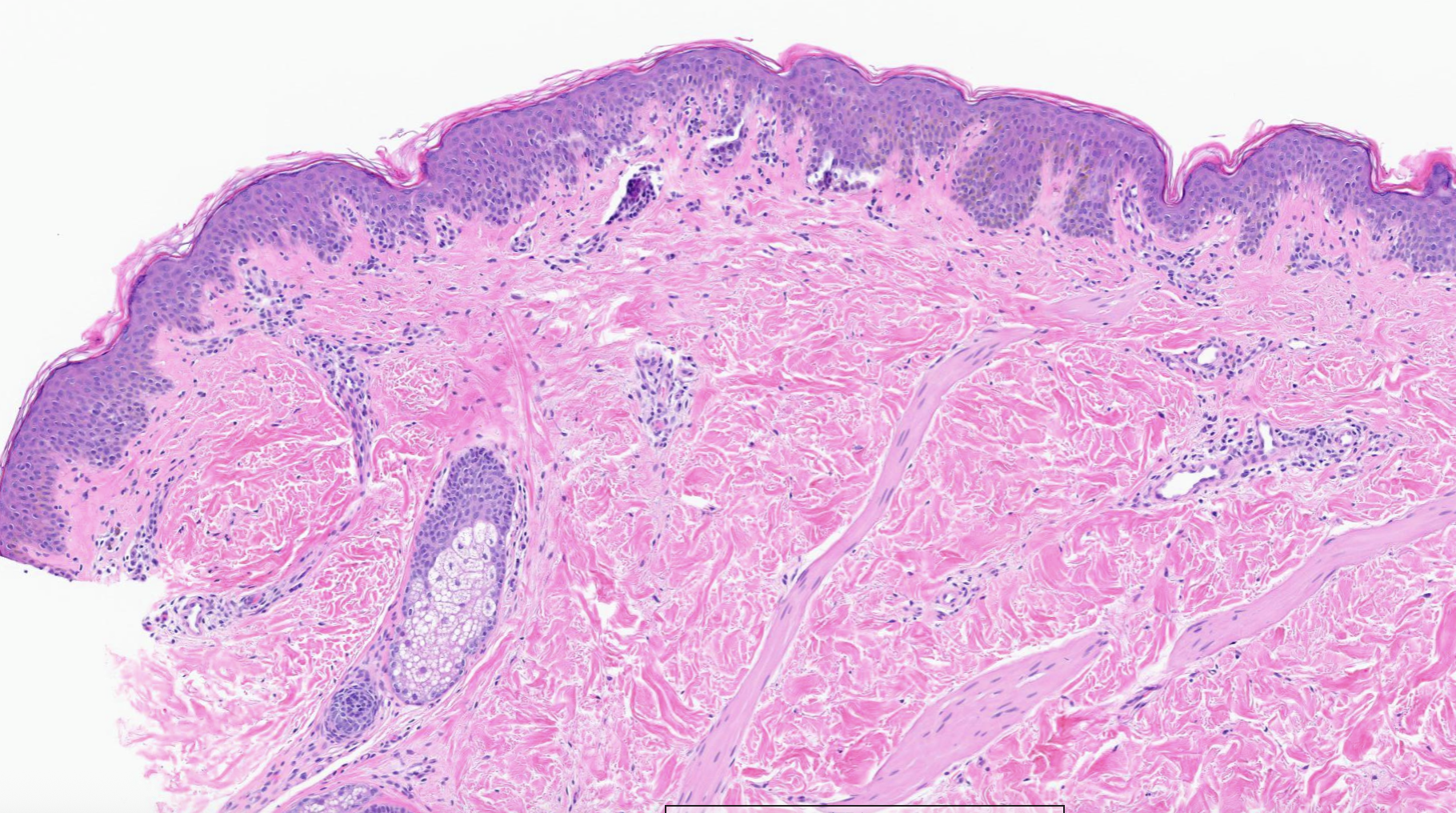
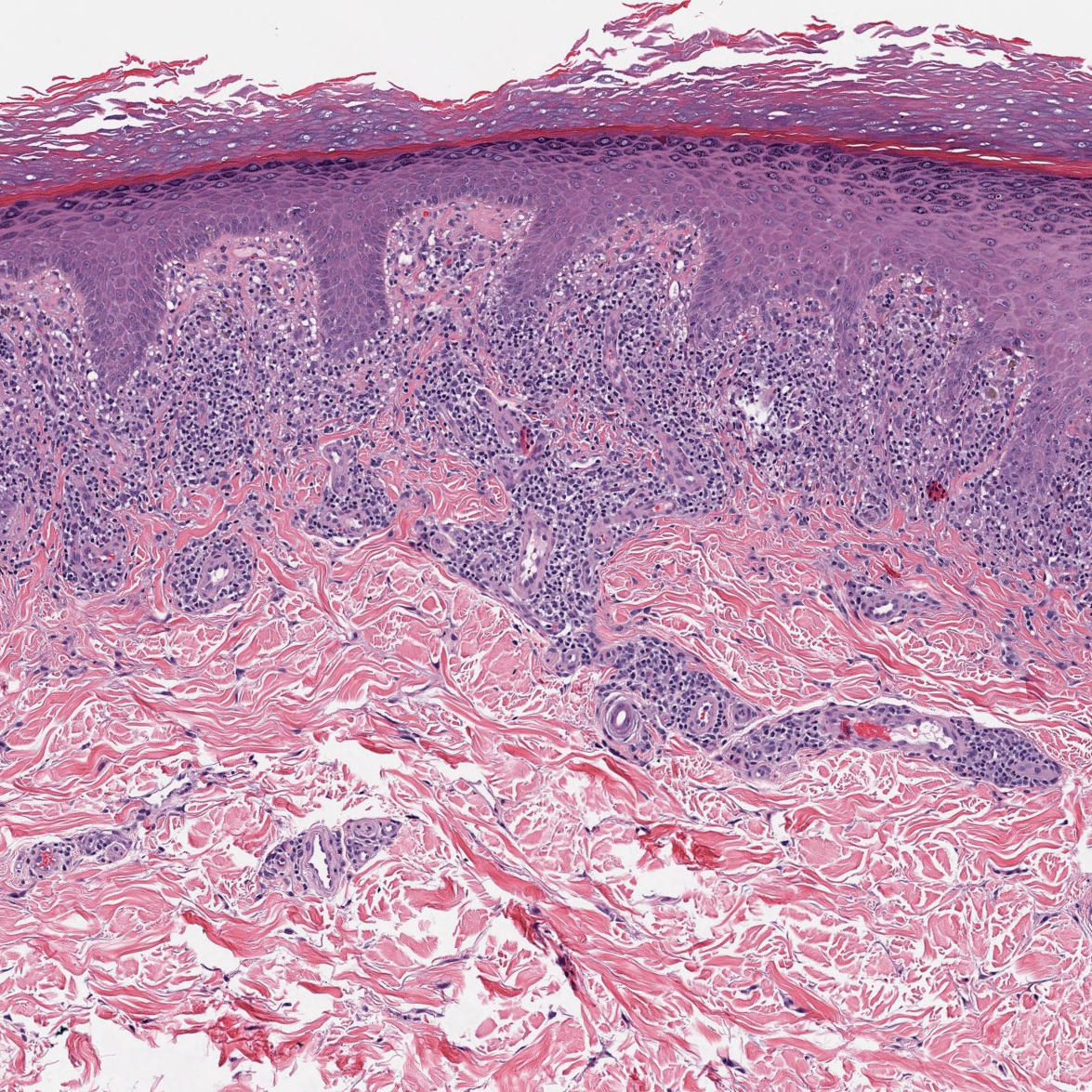
(Image 2: High power showing atypical lymphocytes with perinuclear halos)
Key Histologic Findings
On examination, several defining features stand out:
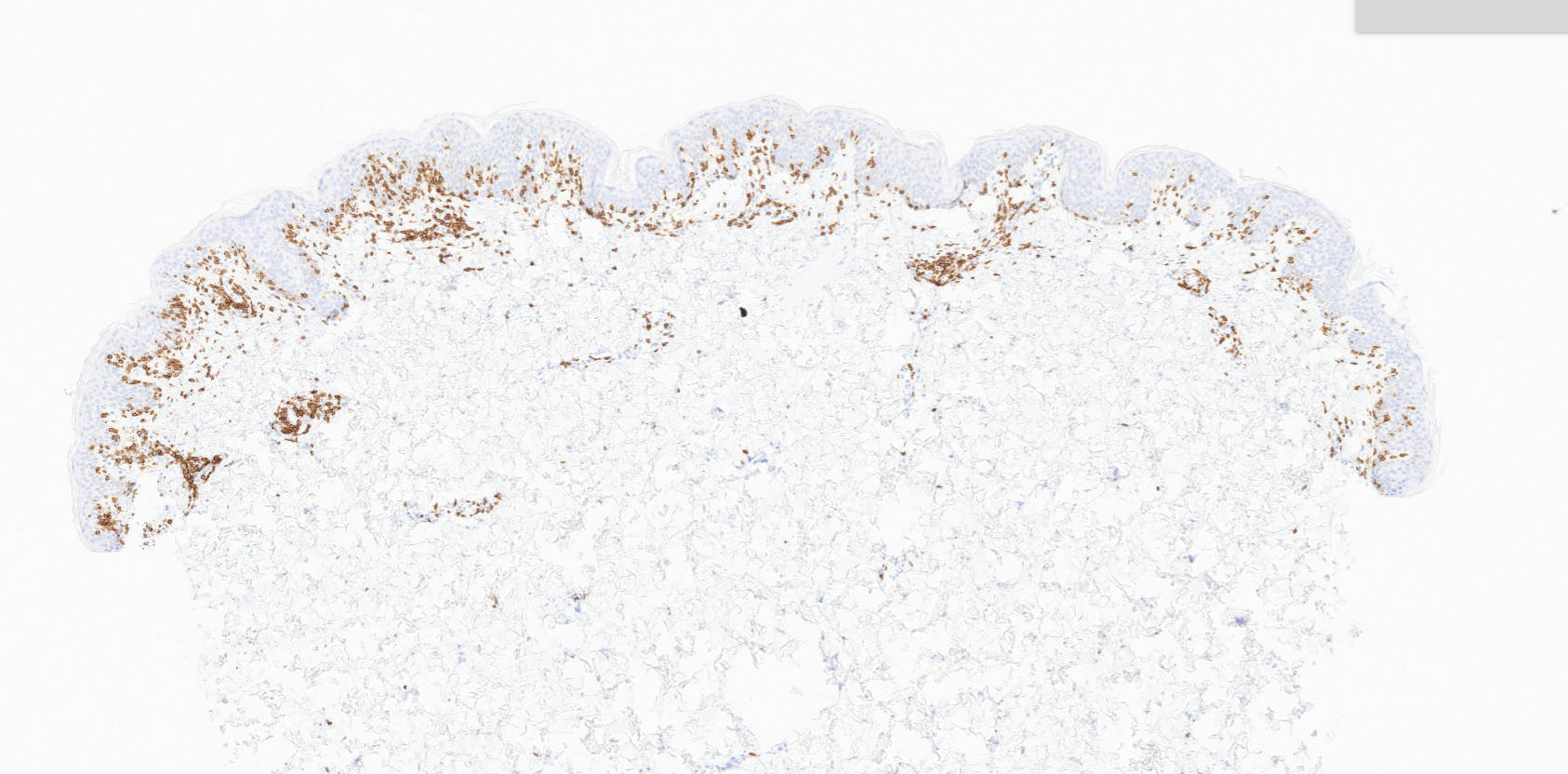
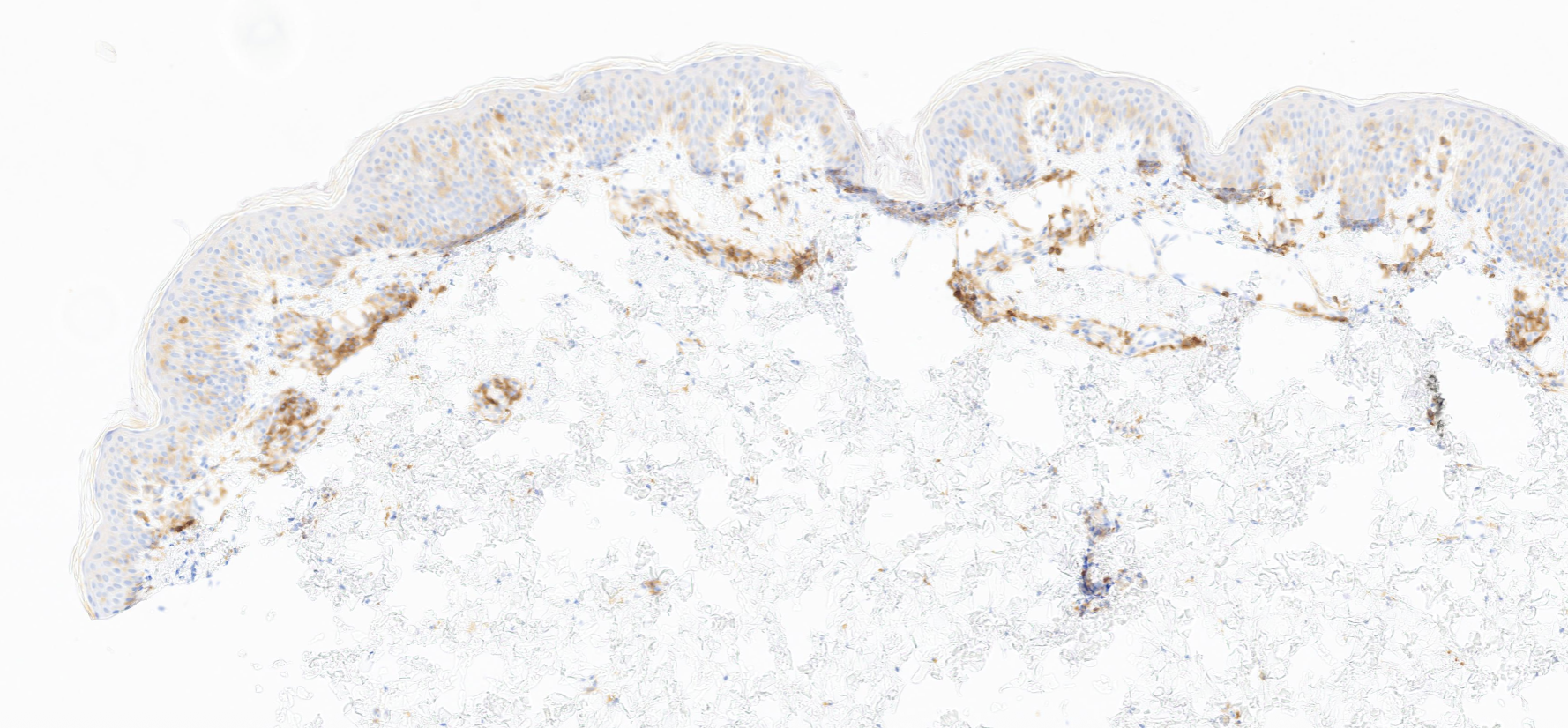
(Image 3: IHC CD3 – Medium power showing epidermotropism)
(Image 4: CD4)
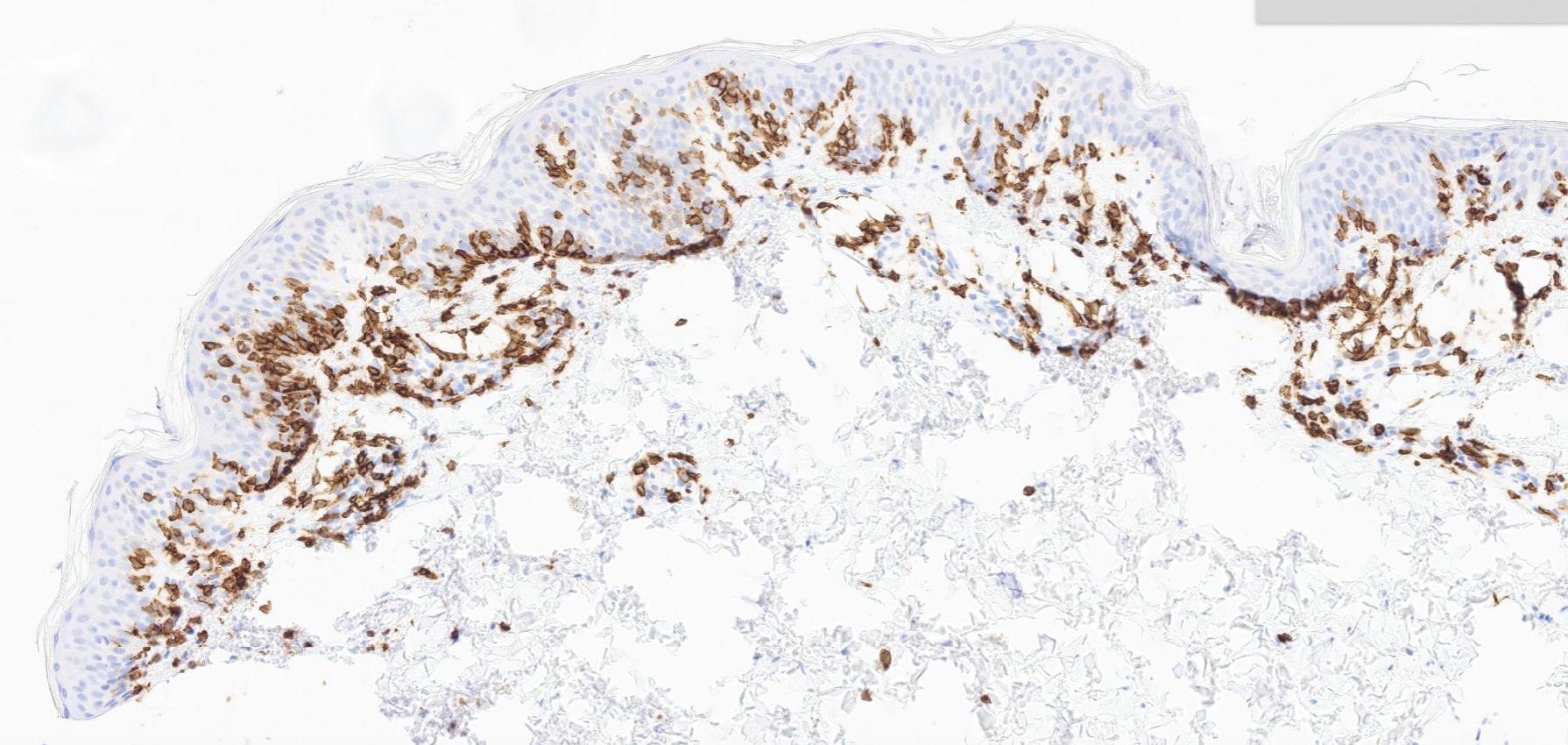
(Image 5: IHC CD8)
Differential Diagnosis: Three Common Mimickers
When evaluating hypopigmented patches in a young patient, several differentials come to mind. Let’s walk through the three most likely contenders and highlight what sets them apart.
Etiology: T-cell mediated lichenoid interface dermatitis; may be idiopathic, drug-induced, or autoimmune
Histology:
Key Distinction: Lichen planus produces a band-like infiltrate at the DEJ with Civatte bodies, but the lymphocytes are mature and polyclonal. CD8+ MF displays nuclear irregularity and epidermotropism with halos — features absent in LP. Immunostains demonstrating a clonal CD8+ T-cell population and TCR gene rearrangement studies confirm MF.
(Image 6: Lichen planus — band-like infiltrate and saw-tooth rete ridges for comparison)
Etiology: Epidermal barrier dysfunction with type 2 immune hypersensitivity; often atopic in origin
Histology:
Key Distinction: Eczema and CD8+ MF can appear deceptively similar at low power, both showing a superficial lymphocytic infiltrate. However, spongiotic dermatitis features spongiosis and lacks the atypical lymphocytes and halo-forming epidermotropism of MF. The absence of T-cell clonality on TCR gene rearrangement studies further supports eczema over MF.
Etiology: Type IV delayed hypersensitivity reaction to a systemically administered medication
Histology:
Key Distinction: Drug eruptions may show interface changes superficially overlapping with patch-stage MF, but the lymphocytes are reactive rather than clonal. Prominent eosinophils and a temporal relationship with a medication favor drug eruption. Drug eruptions resolve with drug withdrawal; CD8+ MF is a T-cell lymphoma requiring ongoing management.
The presence of epidermotropism, atypical lymphocytes with perinuclear halos, and a dominant CD8+ T-cell immunophenotype is diagnostic. This variant is not associated with the typical CD4+ phenotype, setting it apart from conventional MF. Correct identification matters: these patients are often young, and an accurate diagnosis directs appropriate therapy while sparing unnecessary workup for other conditions.
Key Takeaways for Residents:
| Feature | CD8+ Hypo MF | Lichen Planus | Eczema | Drug Eruption |
| Patient profile | Kids, teens, melanated skin | Any age | Any age, atopic | Any age |
| Atypical lymphocytes | ✅ Present | ❌ Absent | ❌ Absent | ❌ Absent |
| Epidermotropism w/ halos | ✅ Present | ❌ Absent | ❌ Absent | ❌ Absent |
| Eosinophils | ❌ Absent | ❌ Rare | ✅ Possible | ✅ Common |
| Spongiosis | ❌ Absent | ❌ Absent | ✅ Present | ✅ Possible |
| CD8+ phenotype | ✅ Dominant | ❌ Mixed | ❌ Mixed | ❌ Mixed |
| T-cell clonality | ✅ Yes | ❌ No | ❌ No | ❌ No |
| Hypopigmentation | ✅ Characteristic | ❌ Not typical | ❌ Not typical | ❌ Not typical |
| Behavior | Indolent MF | Benign / chronic | Benign / chronic | Resolves w/ drug removal |
💬 Final Thought
CD8+ Hypopigmented Mycosis Fungoides is a classic dermatopathology “look-alike” that rewards careful microscopic examination. Remember: the “halos” tell the story.
Sagis Diagnostics is proud to support dermatology residents and dermatology residency programs through high-quality educational content and histopathologic learning resources.
Follow us on Instagram for more micro-learning opportunities with interactive cases and pathology insights.